As indicated in the name, “public” health is primarily shaped and supported through the public sector, i.e., governments. In the U.S., public health powers and responsibilities are shared across federal, state, and local levels of government. Legal authorities for public health powers are derived from the U.S. Constitution and relevant federal, state, and local laws (see Box 2 for an overview of the legal basis for U.S. public health powers). A set of public health departments and agencies at each of these levels forms the organizational backbone of the U.S. public health system. However, many private sector actors such as non-governmental community-based organizations, academic institutions, private companies, philanthropies, and others also have roles in the public health system.
Box 2: Legal Basis for State and Federal Public Health Powers
The U.S. Constitution does not mention public health specifically, but certain powers granted to the federal government and to states in the Constitution have been interpreted as encompassing public health. For example, under the 10th Amendment’s “police powers” clause, states are granted primary responsibility for enacting and enforcing laws to promote the health, safety, and general welfare of people in their jurisdictions, which is understood to include public health. This means that in the U.S., state governments often have primary responsibility for enacting public health measures and deciding on public health policies. During public health emergencies, states also have primary authority to impose and rescind certain measures within their jurisdiction such as business restrictions and school closings.
The Constitution also grants some powers to the federal government. Under the Constitution’s “commerce clause,” the federal government has exclusive authority to regulate interstate and foreign commerce. For public health, this means the federal government has authority to impose quarantines or other health measures that concern the spread of diseases into the U.S. from foreign countries and/or across state lines. The federal government’s Constitutionally derived power to tax and spend for the general welfare provides it the ability to use federal resources in support of public health activities in states and localities nationwide.
Even so, the lines between where federal and state public health powers begin and end – and how these powers are balanced with other legal concerns – are not always perfectly clear and can shift over time. Sometimes, existing rules or practices are challenged in court or changed through new legislation. For example, the Supreme Court in its Jacobson v Massachusetts decision in 1905 established that states can enforce compulsory vaccination laws, setting a precedent that public health concerns can sometimes outweigh individual rights. This and subsequent rulings upholding this principle have been a legal cornerstone for state-level vaccination requirements, such as those for school-aged children. However, in recent years many state legislatures have passed laws intended to weaken vaccination requirements or eliminate them entirely. In addition, during the response to COVID-19, many government-imposed public health interventions such as mandatory masking, social distancing, and vaccination requirements were challenged through legal action.
Federal Government
Each of the three branches of the federal government (Executive, Legislative, and Judicial) has a role in shaping and implementing public health in the U.S.
The President (Executive Branch)
Federal responsibilities and oversight of public health are spread across numerous executive branch agencies and departments overseen by the President (also see “Congress and the Executive Branch and Health Policy). The President, White House, and executive branch agencies also have the authority to set certain aspects of national public health policy, such as determining under which circumstances and for what diseases that individuals entering the U.S. may be subject to quarantine, isolation, and/or other public health measures, invoking border and migration control measures for public health issues such as those allowed under Title 42, and instituting public health controls or other measures on interstate travel and commerce.
The key federal departments and agencies involved in oversight and implementation of public health in the U.S. include:
Department of Health and Human Services (HHS), which has 13 operating divisions and is overseen by a secretary, with multiple assistant secretaries responsible for specific offices and programs. For example, the Office of the Assistant Secretary of Health (OASH) oversees key HHS public health offices and regional offices, as well as the U.S. Public Health Service Commissioned Corps. Also within OASH is the Office of the Surgeon General, which has historically served as a center for expertise on many public health issues and has at times released influential reports, affecting U.S. public health policy and practice in areas such as tobacco, HIV/AIDS, and drunk driving. The following are the core public health-focused operating divisions within HHS:
- Centers for Disease Control and Prevention (CDC) is considered the leading public health agency of the federal government. CDC is comprised of a central Office of the Director, and nine national centers covering different areas of U.S. public health, and a center for global health. CDC houses experts, laboratories, communication services, and other capabilities directed to improve the public’s health and respond to emergencies. One of CDC’s core functions is to support state and local public health efforts through funding and technical assistance. CDC’s budget includes an annually appropriated discretionary amount provided by Congress each year (CDC’s FY2024 enacted budget for its core public health programs was $9.25 billion), and also several programs whose budget is determined by specific Congressionally-mandated program authorizations, such as the Vaccines for Children program (in FY2024 the budget for these mandatory programs totaled $8.03 billion). During outbreaks and other health emergencies, Congress has often provided additional emergency supplemental funding to support CDC response activities. CDC is led by a director, historically appointed by the President without need for Senate confirmation. Due to a law passed by Congress in December 2022, the CDC director position is a Senate-confirmed position as of January 2025.
- Food and Drug Administration (FDA) is responsible for protecting public health by ensuring the safety, efficacy, and security of human and veterinary drugs, biological products, and medical devices. FDA also works to maintain the safety of (some of) the U.S. food supply, cosmetics, and products that emit radiation. FDA review and authorization/approval is necessary for all prescription drugs and all vaccines intended for use in humans, along with many other medical products and health devices. The total program level budget at FDA (the amount of money the FDA can spend for its activities) is comprised of both Congressionally appropriated funds and user fees collected via regulatory review of many of the products under FDA’s purview. In FY2024, the FDA’s total program level budget was $7.2 billion, of which $3.3 billion (46%) came from user fees. FDA is led by a commissioner, a Senate-confirmed position.
- Administration for Strategic Preparedness and Response (ASPR) is an operating division within HHS that leads medical and public health preparedness for, response to, and recovery from disasters and other public health emergencies. This includes activities to support development of medical countermeasures for health emergencies, a stockpile of emergency medical supplies and equipment for use during emergency responses, and support and technical assistance to state and local public health agencies to improve their response capacities. It is comprised of multiple centers, including the Center for Preparedness, the Center for Response, the Center for the Biomedical Advance Research and Development Authority (BARDA), and the Center for the Strategic National Stockpile. ASPR’s operating budget for FY2024 was $3.65 billion. ASPR is led by an Assistant Secretary for Preparedness and Response, a Senate-confirmed position.
- Other HHS Operating Divisions: Other HHS agency programs also play a role in public health, including by helping to build capacity, respond to outbreaks and serve communities, even if they may be more directly focused on clinical care and services, including HRSA’s community health center program and Ryan White HIV/AIDS Program, and SAMSHA’s programs on substance abuse and mental health.
In addition, several other departments and agencies outside of HHS that play a role in promoting the nation’s public health. These include:
- U.S. Department of Agriculture (USDA), which supports U.S. agriculture through assistance to farmers, and also oversees programs aimed at improving health, ending hunger, ensuring food safety, and other areas. USDA also protects public health through regulating aspects of the nation’s food supply, and also providing food services for children and low-income people across the country. USDA’s Food Safety and Inspection Service (FSIS) regulates processors of meat, poultry, and eggs, and helps respond to foodborne disease outbreaks. The department’s Food and Nutrition Service oversees programs to provide food and nutrition education in schools as well as the Supplemental Nutrition Assistance Program (SNAP), which provides food benefits to low-income families.
- Environmental Protection Agency (EPA) helps protect human health related to environmental risks through research and regulation in areas including product safety, indoor air quality, drinking water, and aspects of food safety.
- Department of Defense (DoD) oversees programs focused on the health and safety of active-duty military members and their families, and also supports a number of public health functions such as health surveillance and emergency response.
- Department of Homeland Security (DHS) provides support to help state and local public health agencies improve preparedness and response to terrorism and other public health threats.
- Occupational Safety and Health Administration (OSHA) in the U.S. Department of Labor works to promote safe and healthy working conditions nationwide through setting and enforcing standards, and implementing training, outreach, education, and other assistance programs for worker safety.
- Department of Veterans Affairs (VA) oversees programs focused on the health of military veterans and their families, including public health programs to help promote health and prevent disease in these populations.
This is not meant to be a comprehensive list; other federal agencies also have responsibilities and activities important for public health.
U.S. Congress (Legislative Branch)
Congress (the House of Representatives and the Senate) makes laws, conducts oversight of the Executive branch, and determines the level of federal spending; all roles that are relevant to the U.S. public health system. Much of the federal funding for public health is for discretionary programs rather than mandatory ones (see Funding below), so Congress must come to agreement and pass bills annually to determine how much money goes to these programs. Congress may pass additional, emergency funding to states and localities for public health efforts during national emergencies, such was done numerous times during COVID-19. Congress may also pass laws that change federal practices related to public health, such as a 2022 law that made the CDC director a Senate-confirmed position. Oversight responsibilities for public health in the legislative branch are divided across a number of different Congressional committees with jurisdiction over different aspects of public health policy, and oversight of different Executive branch agencies and departments working in public health.
Federal Courts (Judicial Branch)
U.S. federal courts, up to and including the Supreme Court, pass judgment on how or whether federal public health laws and policies can be carried out and settle disputes between the federal government, individuals, states, and private companies over how public health activities are regulated and implemented. The legal basis for many current public health practices, such as vaccination requirements, rests on federal court decisions and precedents (see Box 2). Federal courts have also weighed in on the legality of a number of federal public health policies enacted during the response to COVID-19, such the CDC masking requirement for public transportation issued in January 2021 that was challenged and ultimately overturned by a federal court in April 2022, and the COVID-19 vaccination mandate for federal workers implemented by the Biden Administration in September 2021 that was ultimately rescinded after legal challenges were raised in federal courts.
State, Local, and Territorial Governments
States are given primary responsibility for many public health powers under the U.S. Constitution (see Box 1). Each of the 50 states plus Washington D.C., five U.S. territories (American Samoa, Mariana Islands, Guam, Puerto Rico, and the Virgin Islands), and three associated states (Marshall Islands, Micronesia, and Palau) have public health departments that are responsible for implementing public health programs in their jurisdictions. Funding for public health programs at the state and local levels comes from a combination of federal, state, and other sources (see funding section below).
Across States, Public Health Governance Varies
How public health is governed differs across these states and territories. Some have a very centralized governance model, where most or all parts of the state are served by local units of the state health agency and primary decision-making powers reside with state representatives. Others have a more decentralized governance structure, where most or all parts of the state are served by local public health agencies that may be independent of the state health agency. Still others have a mixed or shared approach to public health governance between the state and local decisionmakers. A 2022 analysis by the Association of State and Territorial Health Organizations (ASTHO) found that of the 50 states and D.C., 16 are centralized, 27 decentralized, and 8 have a mixed or shared approach to governance (See Figure 2).
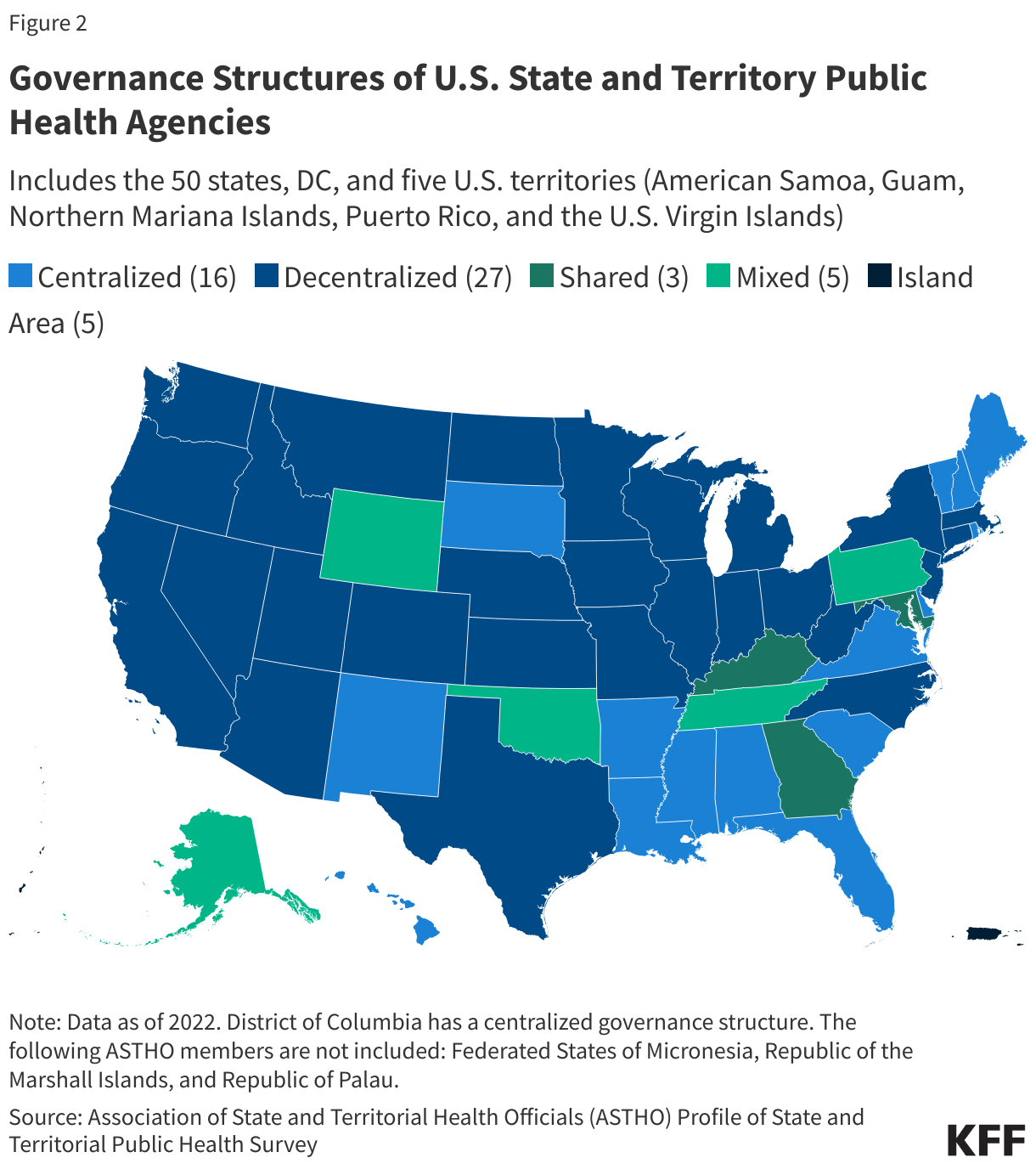
This variation in governance leads to very different processes across states for how public health policy is determined and implemented. While more decentralized public health governance can result in public health programs that are more tailored to the needs of specific areas, it can also make coordinated public health action more challenging, especially during outbreaks and pandemics, as occurred during COVID-19.
Common Public Health Activities at the State Level
According to a 2022 survey conducted by ASTHO, the activities most commonly implemented by state public health agencies in 2022 included:
- communicable disease screening, prevention, and treatment, such as for HIV/AIDS and sexually transmitted diseases (all 51 state health agencies including D.C. provide these services);
- public health surveillance such as tracking chronic and communicable diseases as well as injuries (all 51 state health agencies);
- immunization support, including managing orders and distributing vaccines for children and maintaining a childhood immunization registry (all 51 state health agencies);
- laboratory services such as foodborne illness testing and influenza virus typing (50 state health agencies, all except Kentucky).
Other very common public health activities across states include: chronic disease prevention, family planning, maternal and child health home visits, tobacco cessation and prevention programs, food safety, inspection and training programs, and cancer screenings.
Local and Tribal Health Agencies
Even as state governments have the primary mandate to oversee public health policies and programs, many public health programs within states and territories are implemented through local (such as regional, county, city, and tribal) health departments. According to the National Association of County and City Health Officials (NACCHO), over 3,300 local health agencies are responsible for implementing public health programs across the country. Depending on the governance model present in each state, these local public health departments may have more or less autonomy regarding public health in their jurisdictions. Some areas may have local boards of health authorized by state laws, which establish guidelines for the operation of public health programs in more local level jurisdictions. In addition, under U.S. law, the 574 federally recognized American Indian and Alaska Native tribes and villages have many powers of self-government, which include responsibilities for implementing public health programs. Given this varied approach across states and at the local level, the U.S. is often referred to as having a “patchwork” public health system.
Also important for public health are a wide variety of non-governmental, including community-based, actors. This includes the public health professional associations that often advocate for and represent public health practitioners, such as the aforementioned ASTHO and NACCHO, plus the Council of State and Territorial Epidemiologists (CSTE), the Association of Immunization Managers (AIM), the American Public Health Association (APHA), Trust for Americas Health (TFAH), community-based organizations, philanthropic organizations, and many others. Colleges and universities are also important: there are at least 66 schools of public health, 164 public health programs, and 29 baccalaureate public health programs at institutions of higher learning in the U.S., which support research, training, and education programs in this field. A host of private companies are important for U.S. public health functions, including pharmaceutical and medical device companies, laboratories, and many others.

